Recent studies have found that chronic obstructive pulmonary disease (COPD) is one of the significant factors that affect the death of patients in COVID-19. Among the dead people in COVID-19, the proportion of patients with chronic obstructive pulmonary disease is 6%, but only 1% among the surviving people. In addition, although patients with chronic obstructive pulmonary disease may not be more likely to be infected with Covid-19, they are more likely to die when they are infected.
What is chronic obstructive pulmonary disease? Chronic obstructive pulmonary disease (COPD) is a chronic bronchitis and/or emphysema characterized by airflow obstruction, which can further develop into chronic diseases of cor pulmonale and respiratory failure. Different from common chronic diseases such as hypertension and diabetes, chronic obstructive pulmonary disease is often not well known.
1. The prevalence rate of COPD in men over 70 years old is nearly 50%, and the difference between male and female is nearly 1 time.
According to the latest China Lung Health Survey (CPH2018), among 50,991 people surveyed from June 2012 to May 2015, the prevalence rate of COPD was 8.6%. Based on this, it is estimated that about 99,900 million people in Chinese suffer from COPD. The prevalence rate of COPD increases with age. The prevalence rate of people over 40 years old is significantly higher than that of people aged 20-39. The prevalence rate of COPD in men over 70 years old is nearly 50%. At the same time, the prevalence rate of men in all age groups is higher than that of women, and the prevalence rate of men over 30 years old is more than twice that of women.
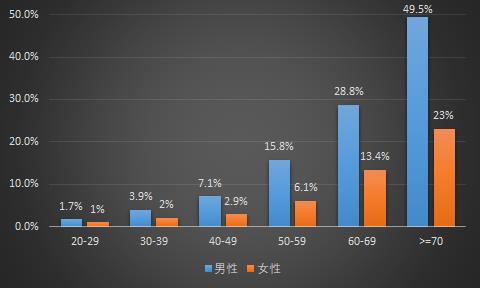
Figure 1: Prevalence of COPD in different gender and age groups.
2. Smoking is the main risk factor, and air pollution is the main risk factor for non-smokers to get sick.
CPH2018 also made a statistical analysis of possible risk factors of COPD, including smoking, air quality, BMI, family history, education, etc. The results showed that smoking, air pollution, low BMI and parents’ history of respiratory diseases were all risk factors of COPD, among which smoking and air pollution were the main risk factors.

Figure 2: odds ratio (OR) of 2:COPD risk factors
Note: odds ratio (OR, Odds ratio) is the ratio of the exposed and unexposed people in the case group divided by the ratio of the exposed and unexposed people in the control group. Greater than 1 indicates that this factor is a risk factor, less than 1 indicates that this factor is a protective factor, and equal to 1 indicates that this factor does not work.
The analysis also shows that smoking history has a significant impact on the overall prevalence of COPD, and the prevalence of COPD increases with the increase of smoking years. Air pollution has no significant effect on the prevalence of COPD in the whole population, but it has a significant effect on non-smoking groups. The more serious air pollution is, the higher the prevalence of COPD is.
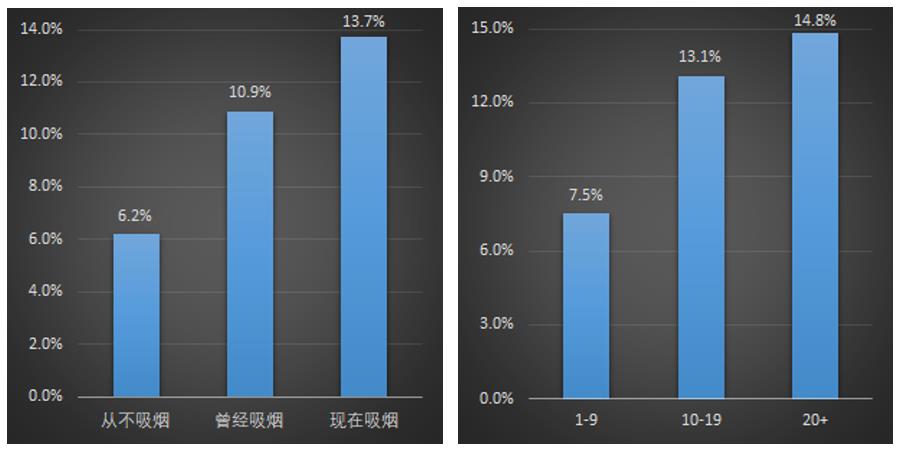
Figure 3: Smoking history and COPD prevalence Figure 4: Smoking years and COPD prevalence.
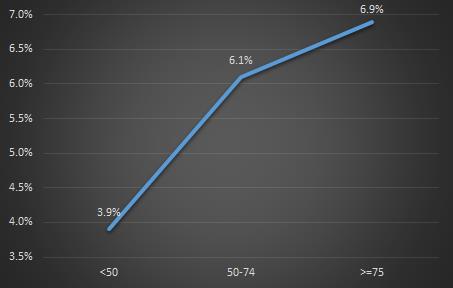
Figure 5: Air quality and COPD prevalence rate
The Prospective Research Project of Chronic Diseases in China also published a survey of 280,000 non-smoking adults in China in 2019. The results show that using solid fuel is an important risk factor for major respiratory diseases, and switching to clean fuel such as natural gas can reduce the risk. Because chronic obstructive pulmonary disease is related to the concentration of sulfur dioxide and carbon monoxide, people who are engaged in jobs with dust environment, such as teachers and coal miners, are also prone to COPD.
3. The prevalence rate of people over 40 years old is different in different regions, with the highest in southwest China (20.2%) and the lowest in central China (10.2%).
The research conducted by China Center for Disease Control and Prevention on 66,752 people in 2014-2015 found that the prevalence rate of COPD over 40 years old also showed obvious differences in different regions, with the highest prevalence rate in southwest China (20.2%) and the lowest in central China (10.2%).
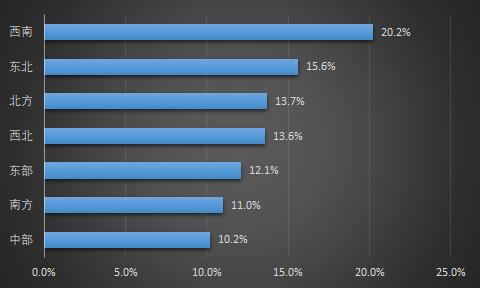
Figure 6: Prevalence rate of COPD among people over 40 years old in different regions.
4. Up to 56% of COPD patients may have cognitive impairment.
A large number of neuropsychological tests suggest that up to 56% patients may have cognitive impairment. The Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD)2021 also pointed out that cognitive impairment is common in COPD patients, and the prevalence and severity vary according to the evaluation type, with an average prevalence of about 32%. Moreover, cognitive impairment will aggravate the health problems of COPD patients. Compared with patients with single disease, patients with cognitive impairment and COPD have a higher respiratory-related hospitalization rate of 48% and a higher mortality rate of 3 times. Therefore, it is particularly necessary to help patients with complications to carry out effective self-management.
In addition, cardiovascular disease, osteoporosis, depression/anxiety are also common and important complications of COPD.
5. The mortality rate of COPD has decreased obviously year by year, but it is still high compared with other developed countries.
The mortality rate of COPD in China decreased from 99/100,000 in 1990 to 68/100,000 in 2017, and the mortality rate of standardized age decreased by 68.6%. Although the mortality rate in China is decreasing year by year, it is still at a high level compared with other developed countries (see the figure below).
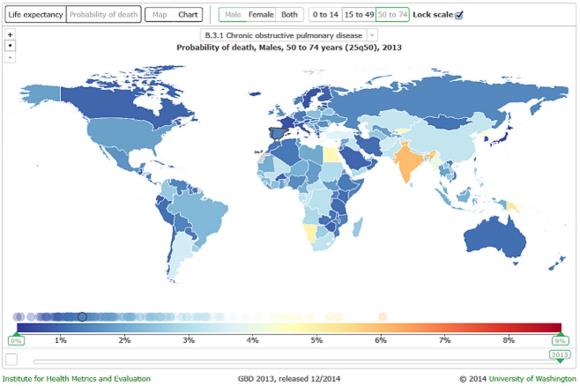
Figure 7: Mortality rate of male COPD patients aged 50-74 in countries around the world.
6. The diagnosis rate is lower than 30%, and the proportion of hospitalization is lower than that of outpatient treatment.
The diagnostic rate of COPD in China is between 23.61% and 30.00%, which shows that the diagnostic rate of COPD in China is low and the missed diagnosis and misdiagnosis are serious. On the one hand, COPD is asymptomatic in the early stage. In epidemiological screening, more than 70% of patients (I~II stage) have little or no symptoms, and even if they have symptoms, they just cough and expectoration, which has not attracted the attention of patients. On the other hand, due to the cost of examination and technical operation, lung function examination, as a gold standard for the diagnosis of COPD, has not been popularized in many hospitals (especially in primary hospitals), resulting in many patients not being diagnosed with COPD in time and delaying treatment.
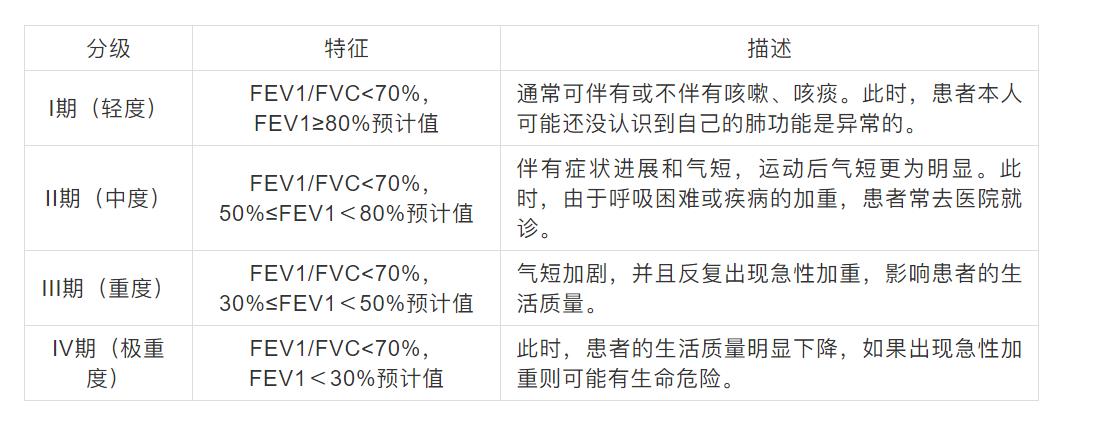
Table 1: COPD pulmonary function staging (GOLD staging) [After inhaling bronchodilator]
In addition, the diagnosis and treatment of COPD in China is also more severe. The conventional treatment rate of COPD patients is only 7.9%, and 84% of patients with stage ⅱ and above have not received treatment. The proportion of COPD patients receiving outpatient treatment is about 50%, while the proportion receiving hospitalization is only between 8.78% and 35.60%.
7. The average medical expenses of COPD ranged from 5,000 yuan to 16,000 yuan.
At present, no scholars have studied the medical expenses of COPD patients nationwide, and most of the research on COPD expenses is limited to local or regional areas.
A study on the medical expenses of COPD patients in Ningbo, Zhejiang Province found that from October 2012 to October 2013, the hospitalization expenses of male patients and female patients are shown in the following table. Among them, the average total hospitalization expense for men is 16,000 yuan, while that for women is 14,500 yuan, and only about 30% is borne by individuals.

Table 2: Hospitalization expenses of COPD patients in Ningbo, Zhejiang Province
In recent years, because the prevalence rate in southwest China is higher than that in other regions, many scholars have begun to choose southwest China to study the treatment cost of COPD patients. The following table is part of the research results, from which we can find that the overall cost of the western region is low, and the average hospitalization cost does not exceed 10 thousand yuan. In addition, according to the survey data of Sichuan province, the cost of western medicine accounts for the highest proportion, accounting for 38.32%, followed by the cost of diagnosis, accounting for 24.41%.

Table 3: Hospitalization expenses of COPD patients in western China
8. About 58% of commonly used drugs for COPD have been included in the medical insurance catalogue.
COPD can be divided into stable stage and acute exacerbation stage according to the progress of the disease course. In the stable stage, the symptoms such as cough and shortness of breath are stable or mild, while in the acute exacerbation stage, the respiratory symptoms that lead to additional treatment are seriously aggravated, and the patients’ cough and wheezing are aggravated, or may be accompanied by fever and other inflammatory manifestations. Drug therapy is a common treatment for COPD. GOLD2021 edition points out that drug therapy can alleviate COPD symptoms and reduce the frequency and severity of acute exacerbation. At present, there are data showing that drug therapy can reduce mortality. It is worth noting that COPD patients need to take drugs for a long time, mainly inhaled drugs, supplemented by oral drugs. With the progress of COPD, the therapeutic drugs and management methods used have been adjusted.
References:
[1] China Pulmonary Health Study Group. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018 Apr 28; 391(10131):1706-1717. doi: 10.1016/S0140-6736(18)30841-9. Epub 2018 Apr 9. PMID: 29650248.
[2] Li G, Liu Y, Jing X, et al. Mortality risk of COVID-19 in elderly males with comorbidities: a multi-country study. Aging (Albany NY). 2020 Dec 31; 13(1):27-60. doi: 10.18632/aging.202456. Epub 2020 Dec 31. PMID: 33472167.
[3] Zhu B, Wang Y, Ming J, et al. Disease burden of COPD in China: a systematic review. Int J Chron Obstruct Pulmon Dis. 2018 Apr 27;13:1353-1364. doi: 10.2147/COPD.S161555. PMID: 29731623; PMCID: PMC5927339.
[4] GBD 2016 Causes of Death Collaborators Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1151–1210.
[5] Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019 Sep 28; 394(10204):1145-1158. doi: 10.1016/S0140-6736(19)30427-1. Epub 2019 Jun 24. Erratum in: Lancet. 2020 Jul 4; 396(10243):26. PMID: 31248666; PMCID: PMC6891889.
[6] Chan K H , Kurmi O P , Bennett D A , et al. Solid Fuel Use and Risks of Respiratory Diseases: A Cohort Study of 280, 000 Chinese Never-Smokers[J]. American Journal of Respiratory and Critical Care Medicine, 2019, 199.
[7] Lowe KE, Regan EA, Crapo JD, et al. COPDGene? 2019: Redefining the Diagnosis of Chronic Obstructive Pulmonary Disease. Chronic Obstr Pulm Dis. 2019 Nov; 6(5):384-399. doi: 10.15326/jcopdf.6.5.2019.0149. PMID: 31710793; PMCID: PMC7020846.
Shi Bijun, Zhang Tao, Cui Jun, Wang Yong, AARON Li. Analysis of direct economic burden of 803 patients with chronic obstructive pulmonary disease in Ningbo community, Zhejiang province [J]. Disease surveillance, 2015,30(4):300-304.
Zhao Hanqing, Li Xinyi, Tank Tan, et al. Analysis of hospitalization expenses of patients with chronic obstructive pneumonia in Sichuan Province [J]. Health Soft Science, 2020, v.34; No.292(05):57-62.
[10] Wang Lianhong, Luo Qian, Zhang Li. Analysis of disease cost of patients with chronic obstructive pulmonary disease in Zunyi area in 2014 [J]. Guizhou Medicine, 2015, 000(011):1048-1049.
[11] Yu Juan. Analysis of hospitalization expenses and influencing factors of patients with chronic obstructive pulmonary disease in Lanzhou urban hospital [D]. Lanzhou: Lanzhou University, 2018.
[12] Zhong Nanshan. Research progress on prevention and treatment of chronic airway diseases in 2017 [J]. West China Medicine, 2018,33(01):1-7.